
What is a traumatic brain injury (TBI)?
A traumatic brain injury (TBI) refers to a brain injury that is caused by an outside force. TBI can be caused by a forceful bump, blow, or jolt to the head or body, or from an object entering the brain. Not all blows or jolts to the head result in TBI.
Some types of TBI can cause temporary or short-term problems with brain function, including problems with how a person thinks, understands, moves, communicates, and acts. More serious TBI can lead to severe and permanent disability, and even death.
Some injuries are considered primary, meaning the damage is immediate. Others can be secondary, meaning they can occur gradually over the course of hours, days, or weeks after injury. These secondary brain injuries are the result of reactive processes that occur after the initial head trauma.
There are two broad types of head injuries: Penetrating and non-penetrating.
-
Penetrating TBI (also known as open TBI) happens when an object pierces the skull (e.g., a bullet, shrapnel, bone fragment, etc.) and enters the brain tissue. Penetrating TBI typically damages only part of the brain.
-
Non-penetrating TBI (also known as closed head injury or blunt TBI) is caused by an external force strong enough to move the brain within the skull. Causes include falls, motor vehicle crashes, sports injuries, blast injury, or being struck by an object.
Some accidents or trauma can cause both penetrating and non-penetrating TBI in the same person.
Signs and symptoms of traumatic brain injury
Headache, dizziness, confusion, and fatigue tend to start immediately after an injury but resolve over time. Emotional symptoms such as frustration and irritability tend to develop during recovery.
Seek immediate medical attention if the person experiences any of the following symptoms, especially within the first 24 hours after an injury to the head:
Physical symptoms of TBI
- Headache
- Convulsions or seizures
- Blurred or double vision
- Unequal eye pupil size or dilation
- Clear fluids draining from the nose or ears
- Nausea and vomiting
- New neurological problems, such as slurred speech, weakness of arms, legs, or face, or loss of balance
Cognitive/behavioral symptoms of TBI
- Loss of or change in consciousness for anywhere from a few seconds to a few hours
- Decreased level of consciousness (e.g., hard to awaken)
- Confusion or disorientation
- Problems remembering, concentrating, or making decision
- Changes in sleep patterns (e.g., sleeping more, difficulty falling or staying asleep, inability to wake)
- Frustration, irritability
Perception and sensation symptoms of TBI
- Light-headedness, dizziness, vertigo, or loss of balance or coordination
- Blurred vision
- Hearing problems, such as ringing in the ears
- Unexplained bad taste in the mouth
- Sensitivity to light or sound
- Mood changes or swings, agitation, combativeness, or other unusual behavior
- Feeling anxious or depressed
- Fatigue or drowsiness; a lack of energy or motivation
TBI in children
Children might be unable to let their caregivers know that they feel different following a blow to the head. It is important for adults to pay attention to a child’s behavior and ask about possible symptoms following a head injury. A child with a TBI may display the following signs or symptoms:
- Changes in eating or nursing habits
- Persistent crying, irritability, or crankiness; inability to be consoled
- Changes in ability to pay attention
- Lack of interest in a favorite toy or activity
- Changes in sleep patterns
- Seizures
- Sadness
- Loss of a skill, such as toilet training
- Loss of balance or unsteady walking
- Vomiting
TBI’s effects on consciousness
A TBI can cause problems with consciousness, awareness, alertness, and responsiveness. Generally, there are four abnormal states that can result from a severe TBI:
-
Minimally conscious state—People in this state still display some evidence of self-awareness or awareness of their environment (such as following simple commands and giving yes or no responses).
-
Unresponsive wakefulness syndrome (UWS)—A result of widespread damage to the brain, people with UWS are unconscious and unaware of their surroundings. However, they can have periods of unresponsive alertness and may groan, move, or show reflex responses.
-
Coma—A person in a coma is unconscious, unaware, and unable to respond to external stimuli such as pain or light. Coma generally lasts a few days or weeks, after which the person may regain consciousness, die, or move into a vegetative state.
-
Brain death—The lack of measurable brain function and activity after an extended period of time is called brain death and can be confirmed by tests that show blood is not flowing to the brain.
How does TBI affect the brain?
TBI-related damage can be confined to one area of the brain, known as a focal injury, or it can occur over a more widespread area, known as a diffuse injury. The type of injury also affects how the brain is damaged. The types of damage usually seen in the brain from a TBI include bleeding, swelling, and tearing that injures nerve fibers. This damage can cause inflammation, swelling, and metabolic changes.
-
Diffuse axonal injury (DAI), one of the most common types of brain injuries, refers to widespread damage to the brain's white matter. DAI commonly occurs in auto accidents, falls, or sports injuries. It can disrupt and break down communication among nerve cells in the brain. It also leads to the release of brain chemicals that can cause further damage. Brain damage may be temporary or permanent and recovery can take a long time.
-
Concussion is a type of mild TBI that may be considered a temporary injury to the brain but could take minutes to several months to heal. Concussion may be caused by a blow to the head, a sports injury or fall, a motor vehicle accident, or a rapid movement of the brain within the skull, as can happen when a person is violently shaken. The individual with concussion either suddenly loses consciousness or their state of conscious or awareness changes suddenly. A second concussion closely following the first one—the so-called “second hit” phenomenon—and can lead to permanent damage or even death in some instances. Post-concussion syndrome involves symptoms that last for weeks or longer.
-
Image
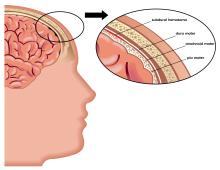
Hematomas are bleeding in and around the brain caused by a burst blood
vessel. Different types of hematomas form depending on where the blood collects in the protective membranes surrounding the brain, which include the dura mater (outermost), arachnoid mater (middle), and pia mater (innermost).
-
Epidural hematomas involve bleeding into the area between the skull and the dura mater. These can occur within minutes to hours after injury and are particularly dangerous.
-
Subdural hematomas involve bleeding between the dura and the arachnoid mater, and, like epidural hematomas, exert pressure on the outside of the brain. They are very common in older adults after a fall.
-
Subarachnoid hemorrhage is bleeding between the arachnoid mater and the pia mater.
-
Intracerebral hematoma involves bleeding into the brain itself and damages the surrounding tissue.
-
- Contusions are a bruising or swelling of the brain that occurs when very small blood vessels bleed into brain tissue. Contusions can occur directly under the impact site (a coup injury) or, more often, on the complete opposite side of the brain from the impact (a contrecoup injury). They can appear after a delay of hours to a day. These generally occur when the head abruptly decelerates, which causes the brain to bounce back and forth within the skull (such as in a high-speed car crash or in shaken baby syndrome).
-
Skull fractures are breaks or cracks in one or more of the bones that form the skull. They are a result of blunt force trauma and can cause damage to the membranes, blood vessels, and brain under the fracture. Helmets can help prevent skull fractures.
-
Chronic traumatic encephalopathy (CTE) is a progressive neurological disorder with symptoms that may include problems with thinking, understanding, and communicating; movement disorders; problems with impulse control and depression; confusion; and irritability. CTE occurs in those with extraordinary exposure to multiple blows to the head. It develops over many years and can take years to show symptoms. Studies of retired boxers have shown that repeated blows to the head can cause issues including memory problems, tremors, lack of coordination, and dementia. Recent studies have demonstrated cases of CTE in other sports with repetitive mild head impacts (e.g., soccer, wrestling, football, and rugby).
-
Post-traumatic dementia (PTD) can arise after a single, severe TBI. PTD may be progressive and share some features with CTE. Studies assessing patterns among large populations of people with TBI indicate that moderate or severe TBI in early or mid-life may be associated with increased risk of dementia later in life.

The initial damage to the brain described above can itself cause secondary damage. Secondary damage refers to the changes occur over a period of hours to days after the primary brain injury. Examples of secondary damage include:
-
Hemorrhagic progression of a contusion (HPC) are injuries that occur when a contusion continues to bleed in and around the brain and expand over time. This creates a new or larger lesion and leads to swelling and further brain cell loss.
-
A breakdown in the blood-brain barrier refers to the disruption of the network that controls the movement of cells and molecules between the blood and fluid that surrounds the brain's nerve cells. Once the blood-brain barrier is disrupted, blood, plasma proteins, and other foreign substances leak into the space between neurons in the brain and trigger a chain reaction that causes brain swelling. It also causes inflammatory responses which can be harmful to the body if they continue for an extended period of time and the inappropriate release of neurotransmitters, which can damage or kill nerve cells.
-
Increased intracranial pressure is usually caused by brain swelling inside the skull as a result of the injury. This pressure can damage brain tissue and prevent blood flow to the brain, depriving it of the oxygen it needs to function.
Other secondary damage can be caused by infections to the brain, low blood pressure or oxygen flow as a result of the injury, hydrocephalus, and seizures.
Who is more likely to get a traumatic brain injury?
Adults age 65 and older are at greatest risk for being hospitalized and dying from a TBI, most often from a fall. In every age group, serious TBI rates are higher for men than for women. Men are more likely to be hospitalized and are nearly three times more likely to die from a TBI than women.
The leading causes of TBI include:
-
Falls—According to the Centers for Disease Control and Prevention (CDC), falls are the most common cause of TBIs and occur most frequently among the youngest and oldest age groups.
-
Blunt trauma accidents—Accidents that involve being struck by or against an object, particularly sports-related injuries, are a major cause of TBI.
-
Vehicle-related injuries—Pedestrian-involved accidents, as well as accidents involving motor vehicles and bicycles, are the third most common cause of TBI.
-
Assaults/Violence—Abuse-related TBIs are head injuries that result from intimate partner violence, assaults, shaken baby syndrome, and wounds to the head caused by gunshots or other weapons.
-
Explosions/Blasts—TBIs caused by blast trauma from roadside bombs have become a common injury to service members in military conflicts. The majority of these TBIs are classified as mild head injuries.
How is a traumatic brain injury diagnosed and treated?
Preventing TBI
The best treatment for TBI is prevention. Unlike most neurological disorders, head injuries can be prevented. The following actions can help prevent TBI:
- Wear a seatbelt
- Wear a helmet when riding a bicycle, skateboarding, and playing sports like hockey and football. Make sure it is the appropriate helmet for the activity and that it fits correctly.
- Never drive under the influence of drugs or alcohol
- Improve balance and strength with a regular physical activity program
- Make changes in the home to prevent falls:
- Install window guards and safety gates for young children
- Improve lighting and remove rugs, clutter, and other trip hazards in hallways
- Use nonslip mats and install grab bars next to toilets and in tubs or showers, especially for older adults
- Install handrails on stairways
Diagnosing TBI
All TBIs should be evaluated immediately a professional who has experience with head injuries. A neurological exam will judge motor and sensory skills and test hearing and speech, coordination and balance, mental status, and changes in mood or behavior, among other abilities.
Screening tools developed for coaches and athletic trainers can identify the most concerning concussions for medical evaluation.
Medical providers can use brain imaging to evaluate the extent of the primary brain injuries and determine if surgery will be needed to help repair any damage to the brain. A physical examination by a doctor and the person's symptoms will help determine whether imaging is needed. Commonly used imaging for TBI includes CT (computed tomography) and MRI (magnetic resonance imaging). CT imaging can show a skull fracture and any brain bruising, bleeding, or swelling. MRI is more sensitive and can pick up more subtle brain changes that a CT scan may miss.
Significant advances have been made in the last decade to detect milder TBI damage via imaging. For example, diffusion tensor imaging can identify white matter tracts, fluid-attenuated inversion recovery can detect small areas of damage, and susceptibility-weighted imaging can identify even small and hard to detect brain bleeds. Despite these improvements, currently available imaging technologies, blood tests, and other measures cannot always diagnose mild concussive injuries.
Neuropsychological tests to gauge brain functioning are often used along with imaging in people who have suffered mild TBI. Such tests involve performing specific tasks that help assess memory, concentration, information processing, executive functioning, reaction time, and problem solving.
Many athletic organizations recommend establishing a baseline picture of an athlete's brain function at the beginning of each season, ideally before any head injuries occur. Brain function tests yield information about an individual's memory, attention, and ability to concentrate and solve problems. Brain function tests can be repeated at regular intervals (every one to two years) and also after a suspected concussion. The results may help healthcare providers identify any effects from an injury and allow them to make more informed decisions about whether a person is ready to return to their normal activities.
Treating TBI
Many factors—including the size, severity, and location of the brain injury—influence how TBI is treated and how quickly a person might recover. Although brain injury often occurs at the moment of head impact, much of the damage related to severe TBI develops from secondary injuries which happen days or weeks after the initial trauma. For this reason, people who receive immediate medical attention at a certified trauma center tend to have the best health outcomes.
Genetics may play a role in how quickly and completely a person recovers from a TBI. For example, researchers have found that apolipoprotein E ε4 (ApoE4) — a genetic variant associated with higher risks for Alzheimer's disease — is associated with worse health outcomes following a TBI. Much work remains to be done to understand how genetic factors, as well as specific types of head injuries, affect recovery.
Studies suggest that age and the number of head injuries a person has suffered over his or her lifetime are two critical factors that impact recovery. Brain swelling in newborns, young infants, and teenagers often occurs much more quickly than it does in older people. Evidence from very limited CTE studies suggest that younger people (ages 20 to 40) tend to have more behavioral and mood changes with CTE, while those who are older (ages 50+) tend to have more cognitive difficulties.
Compared with younger adults with the same TBI severity, older adults are more likely to have lasting symptoms. Older people often have other medical issues and may be taking multiple medications, which may complicate treatment. For example, blood thinning medications may increase the risk of bleeding in the brain.
Mild TBI
Some people with mild TBI (such as a concussion) may not require treatment other than rest and over-the-counter pain relievers. Treatment should focus on symptom relief and “brain rest.” Brain rest means avoiding activities that require concentration or attention. The person should be monitored by their healthcare provider to note new or worsening symptoms.
Children and teens who have a sports-related concussion should stop playing immediately and return to play only after being approved by a concussion specialist.
Preventing future concussions is critical. While most people recover fully from a first concussion within a few weeks, the rate of recovery from a second or third concussion is generally slower.
Even after concussion symptoms go away, people should return to their daily activities gradually, and only once they have permission from a doctor. While there are some guidelines available, further research is needed to better understand the effects of mild TBI on the brain and determine when it is safe to resume normal activities.
People with mild TBI should:
-
Make an appointment for a follow-up visit with their healthcare provider to confirm the progress of their recovery
-
Inquire about new or ongoing symptoms and how to treat them
-
Pay attention to any new signs or symptoms even if they seem unrelated to the injury (for example, mood swings, unusual feelings of irritability). These symptoms may be related even if they occurred several weeks after the injury.
Medications to treat symptoms of TBI may include:
-
Over-the-counter or prescribed pain medicines
-
Anticonvulsant drugs to treat seizures
-
Anticoagulants to prevent blood clots
-
Diuretics to help reduce fluid buildup and reduce pressure in the brain
-
Stimulants to increase alertness
-
Antidepressants and anti-anxiety medications to treat depression and feelings of fear and nervousness
Severe TBI
Immediate treatment for someone who has a severe TBI focuses on preventing death; stabilizing the person's spinal cord, heart, lung, and other vital organ functions; ensuring proper oxygen delivery and breathing; controlling blood pressure; and preventing further brain damage. Emergency care staff will monitor the flow of blood to the brain, brain temperature, pressure inside the skull, and the brain's oxygen supply.
A person with severe TBI may need surgery to relieve pressure inside the skull, remove debris, dead brain tissue, or hematomas, or repair skull fractures. While in the hospital for severe TBI, the person should be monitored for infection (particularly pneumonia) and deep vein thrombosis (blood clots that can form during long periods of inactivity).
Rehabilitation for severe TBI
Once their injuries are treated and stabilized in the hospital, people with severe TBI are often transferred to a rehabilitation center where a multidisciplinary team of health care providers help with recovery. The rehabilitation team may include neurologists, nurses, psychologists, and nutritionists, as well as physical, occupational, vocational, speech, and respiratory therapists.
Therapy is aimed at improving the person's ability to perform activities of daily living and to address cognitive, physical, occupational, and emotional difficulties. Treatment may be needed on a short- or long-term basis.
Cognitive rehabilitation therapy (CRT) is a strategy aimed at helping individuals regain their normal brain function through an individualized training program. Using this strategy, people also may learn strategies for coping with persistent memory, problem solving, and thinking problems.
What are the latest updates on traumatic brain injury?
NINDS, a component of the National Institute of Health (NIH), conducts and supports a wide range of basic, clinical, and translational research on TBI. Other NIH institutes also support TBI research.
NINDS-funded research includes studies to understand TBI and its associated conditions, studies to improve diagnosis and outcomes, and studies to develop potential therapies for TBI. Projects are currently:
-
Exploring ways to promote the brain's innate ability to adapt and repair itself, known as neuroplasticity.
-
Refining diagnostic criteria for both CTE and the associated Traumatic Encephalopathy Syndrome (TSE).
-
Supporting the development and validation of clinically relevant biomarkers (signs that may indicate risk of a disease and aid in diagnosis) for TBI through the Translational Outcomes Project in Neurotrauma (-NT) consortium.
-
Identifying biomarkers for CTE in order to detect this and similar disorders in living people rather than through autopsy after death.
Clinical research
NINDS co-leads the Strategies to Innovate EmeRgENcy Care Clinical Trials (SIREN) network. This network supports projects that include TBI trials—one of which is BOOST3 (Brain Oxygen Optimatization in Severe TBI), in which scientists are comparing two methods for monitoring brain tissue oxygen to determine the best treatment approach for people with TBI.
The recently completed NINDS-funded Transforming Research and Clinical Knowledge in TBI, or TRACK TBI, project was an observational study of adults and children with TBI at all levels of injury severity. It provided a TBI database as well as tools and resources to establish more precise methods to diagnose TBI and improve ways to assess a person’s outcomes after an injury. Now, researchers are extending the study by continuing to follow study participants in an effort to identify risk factors and biomarkers for TBI and to learn more about outcomes for individuals with TBI.
Harnessing the efforts of the many physicians and scientists working on developing better treatments for TBI requires that everyone collect the same types of data, including details about injuries and treatment results. NINDS's Common Data Elements project brings the research community together to develop data collection standards.
Scientific collaboration in TBI research
NINDS and the European Commission conduct studies through the International Initiative for TBI research (InTBIR), which seeks to improve diagnosis and evaluate which types of care are associated with the best outcomes in children and adults.
NIH and the Department of Defense together lead the Federal Interagency TBI Research (FITBIR) database, which includes data from observational and other studies.
NIH investigators and the FDA are active collaborators in the Department of Defense-led TBI Endpoints Development (TED) program to develop better designed clinical trials to lead to effective treatments for TBI.
NINDS also works with Department of Defense and the Departments of Health and Human Services, Veterans Affairs, and Education to coordinate TBI research for military members. The associated National Research Action Plan (NRAP) aims to improve prevention, diagnosis, and treatment of TBI and other conditions (such as PTSD) that affect veterans and their families.
To advance research on TBI, it is important that classification of the types of TBI is precise, and evidence-based, beyond the currently used "mild," "moderate," and "severe," designations. To support these efforts, in January 2024, NINDS held the TBI Classification and Nomenclature Workshop.
NIH research projects on TBI can be found using NIH RePORTER, a searchable database of current and past research projects supported by NIH and other federal agencies. RePORTER also includes links to publications from these projects and other resources.
How can I or my loved one help improve care for people with traumatic brain injury?
Consider participating in a clinical trial so clinicians and scientists can learn more about TBI and related disorders. Clinical research with human study participants helps researchers learn more about a disorder and perhaps find better ways to safely detect, treat, or prevent disease.
All types of participants are needed—those who are healthy or may have an illness or disease—of all different ages, sexes, races, and ethnicities to ensure that study results apply to as many people as possible, and that treatments will be safe and effective for everyone who will use them.
For information about participating in clinical research visit NIH Clinical Research Trials and You. Learn about clinical trials currently looking for people with TBI at Clinicaltrials.gov.
People with a TBI also can support research by designating the donation of brain tissue before they die. Human brain tissue is essential to increasing the understanding of how the nervous system functions. The NIH NeuroBioBank is an effort to coordinate the network of brain banks it supports across the country to advance research through the collection and distribution of post-mortem brain tissue to qualified research teams.
Where can I find more information about traumatic brain injury (TBI)?
Information may be available from the following resources: